

8 Reasons not to Vaccinate Your Children against Covid


I’ve written about Covid vaccines for children before but as my country, Ireland, begins to distribute them to even younger children, it merits a revisit. Generally, I try to steer clear of recommending anyone to either take or not take a vaccine and I’ll continue that practice here. However, such is the weight of pressure being directed at parents to put their children forward, I think, for balance, that a list of reasons why you might consider not vaccinating them is reasonable. So here are 8 reasons with sources and links throughout.
(There are plenty of avenues I could go down but I will restrict myself here to clear, verifiable and documented information. As ever, the decision is yours and yours alone.)
1. The Vaccines are not Fully Approved
It’s important not to lose sight of this. Whatever sleight of hand trick the FDA pulled back in August by granting full approval to a completely unavailable version of the Pfizer-Biontech vaccine for adults called “Comirnaty”, that is legally, if not biologically, unique from the one that is continuing to be injected into hundreds of millions of arms under an Emergency Use Authorisation should not distract from the fact that there is no fully approved Covid-19 vaccine for anyone under 16 years of age.1
In the EU, the vaccines are distributed under a “Conditional Marketing Authorisation”. In the UK, it is a “Rapid Temporary Regulatory Approval”. And in the US, as above, it is an “Emergency Use Authorisation”. Consider this carefully as you read on. These are not established vaccines. They represent a remarkable new technology that is a complete departure from traditional approaches. Whereas conventional vaccines merely introduce a dead or attenuated form of a virus into your body that your immune system then builds antibodies against to offer future protection, the mRNA vaccines use an RNA sequence which instructs your own cells to produce part of the SARs-CoV II virus, namely the spike protein. Instead of using the actual virus, mRNA vaccines force your body to become a pathogen producer. Once produced, the theory is that your immune system reacts to the spike protein you produced and builds antibodies needed for protection.
This is amazing science. Ultimately, it could be very useful but don’t let anyone tell you these are normal vaccines. This is a brand new biotechnology. Developing it and trialling it over long periods of time to fully understand the impacts of hijacking your body’s cellular production process makes sense. Injecting it into a whole population of children, who are at virtually zero risk from the disease it seeks to offer protection from, does not. Ask yourself: “Under what circumstances should I consider giving my child a new, unapproved biotechnology like this?” Can you honestly say that those circumstances, whatever you deem them to be, exist today?
2. The Trials are Weak
In a previous essay, I noted that the Clinical Trial conducted by Pfizer for the use of its vaccine in the 12-15 year old category was short and underpowered and it failed to detect the higher incidence of myocarditis that only came to light after it was administered to the public.
The Trial for 5-11 year olds was even worse. It was similarly short and underpowered with no realistic likelihood that that the mere 2,268 participants would help detect rare side-effects. However, the worst part is that it demonstrated zero clinical efficacy of the vaccine. That is, it was not shown to prevent any severe cases, deaths, or hospitalisations. This is largely because Covid does not cause severe cases, deaths or hospitalisations in this age cohort. Half the participants in the trial were given the vaccine and half were given a placebo and then they looked to see who got sick. However, almost no one got sick, vaccinated or not, because, as we shall discuss below, children are generally not seriously affected by Covid.
The press reporting of the trial makes this clear:
“Pfizer’s press release did not include any data on the extent to which the vaccine reduced the chances that children would become sick. (William) Gruber (Pfizer VP) said that there were not enough cases of illness to tell.”2
Essentially, they are basing their hope in the vaccine for this age cohort on antibody counts in the vaccinated trial participants, not any kind of real-world evidence. They are guessing, in other words.
3. Covid Risk for Children is Miniscule
As indicated in the results of Pfizer’s trial, Covid is not a disease of consequence to children. A huge German study found zero deaths from Covid among healthy children between the ages of 5 and 18 years in the first 15 months of the pandemic. Zero. Out of a population of 10.5 million children.
The study concluded:
“Overall, the SARS-CoV-2-associated burden of a severe disease course or death in children and adolescents is low. This seems particularly the case for 5-11-year-old children without comorbidities.”
In Sweden, a country that kept its schools open and its kids unmasked, the data is similar. Up to the end of December 2020, they found zero deaths with Covid among children and concluded a 1 in 130,000 ICU hospitalisation rate.
“Despite Sweden’s having kept schools and preschools open, we found a low incidence of severe Covid-19 among schoolchildren and children of preschool age during the SARS-CoV-2 pandemic. Among the 1.95 million children who were 1 to 16 years of age, 15 children had Covid-19, MIS-C, or both conditions and were admitted to an ICU, which is equal to 1 child in 130,000.”
A UK study found a total of six Covid-19 deaths among young people <18 years of age with no other underlying condition. That is out of a population of 12 million children. That study concluded:
“SARS-CoV-2 is very rarely fatal in CYP (children and young people), even among those with underlying comorbidities. These findings are important to guide families, clinicians and policy makers about future shielding and vaccination.”
In the US, the data is not separated between healthy children and those with comorbidities, however, even grouping all children together it is clear that the Covid disease burden is less than influenza for young people. The CDC has recorded a total of 678 deaths from Covid in all children up to the age of 17 years over nearly two years, including those with severe comorbidities.3 That is out of a population of 73.1 million children. The average flu deaths recorded by the CDC for just one year in this age category is 461 (multiply this by the period over which the Covid deaths are counted: 1.75 years and you get 806). This influenza fatality rate, I will note, has strangely decreased since I checked it last - the CDC seem to be reducing their estimates of paediatric influenza deaths from past seasons and have a note on their website to this effect. Nevertheless, the updated rate is still higher than the Covid mortality rate so the point stands that flu (even with an established vaccine) is more dangerous to children than unvaccinated Covid.
In Ireland, this page from the Health Service Executive (HSE) of Ireland listed the risk of hospitalisation for children from Covid-19 as being 1 in 100,000.

That reference has now been removed after I, and others, pointed out that it was a significantly lower risk to children than the one posed by the vaccine in the form of myocarditis for young boys which the HSE published on the very same webpage:

That reference too has been removed. The page now simply contains vague statements - the risk of hospitalisation is “low”, severe illness is “rare”. Meanwhile, the myocarditis figures have been obfuscated by the use of wider and less relevant age cohorts (up to 29 years of age). Even so, the figures presented (1 in 38,000 and 1 in 17,500) are still higher than the redacted 1 in 100,000 Covid hospitalisation figure.
We’ll talk more about myocarditis shortly but for now, let’s conclude our analysis of paediatric Covid mortality and illness by recognising that it is exceptionally rare. The US figures shows that serious outcomes appear less frequently than flu and the German, Swedish, and British data shows that when it does occur it generally or nearly exclusively occurs in unfortunate children with other serious health issues that, in many cases, will likely have been the actual cause of their death.
All of this lead the American Council on Science and Health to produce this chart displaying the Covid Infection Fatality rate by age (and sex).

As you can see, it doesn’t go above 0.003% in any cohort under 19 years of age. This is a statistically non-existent threat, akin to the kinds of colds children get every year. Aside from obvious things like cancer, heart disease, and flu there is more risk to a child from car accidents, firearm discharges, suffocation, drowning, and fire/burns.4
Does this necessitate emergency products?
4. Long Covid is not a Risk
What can one say about Long Covid - an entirely hypothetical concept based on subjective self-assessments from people who have been psychologically tormented for months and years by a global atmosphere of plague and fear? Long Covid is so ephemeral, so nebulous that it’s difficult to actually grasp anything to disprove.
That said, the Office for National Statistics (ONS) in the UK conducted a survey of almost 27,000 people and discovered that the long list of symptoms associated with Long Covid (fever, headache, muscle ache, weakness or tiredness, nausea or vomiting, stomach pain, diarrhoea, sore throat, cough, shortness of breath, loss of taste and loss of smell) were only slightly less prevalent in people who had not tested positive for Covid as people who had previosuly tested positive (3.4% vs 5%).5 In essence, the symptoms are so vague and widespread that they are indistinguishable from the kind of complaints that are regularly reported by the general population regardless of Covid status.
The ONS’s survey is in keeping with a study from Germany which essentially found the same thing. It concluded:
“There was no statistical difference comparing the reported symptoms between seropositive students and seronegative students. Whether the infection was known or unknown to the participant did not influence the prevalence of symptoms.”
Long Covid is a shadow on a wall, something that seems scary until you shine a light on it and realise there’s nothing actually there.
5. The Vaccines do not stem transmission
I won’t labour this point as it has become fairly obvious at this stage. The White House’s senior Covid advisor, Anthony Fauci, declared back in the summer of 2021 that:
“When you look at the level of virus in the nasopharynx of a vaccinated person who gets a breakthrough infection with Delta, it is exactly the same as the level of virus in an unvaccinated person who's infected.”6
That was in relation to Delta. Omicron is, we are told, even more infectious again particularly in relation to vaccinated people. See below graphs from Ontario and Iceland suggestive that Omicron infects vaccinated people at higher rates than the unvaccinated.


Ultimately, whether Omicron has mutated to be more infectious to vaccinated people is not important here. What is important is that the real-world data does not in anyway support the idea that Covid vaccines reduce transmission. Quite simply, if they did, heavily vaccinated places like Ireland would be seeing less cases, not more.

This matters because given the lack of consequence to children from Covid, the main argument for vaccinating them was to prevent them acting as vectors for the virus to reach vulnerable people. The clear failure of the vaccines to achieve such a result renders that argument completely obsolete.
6. The Risk of Vaccines for Children is higher than from Covid
Returning to Ireland’s HSE and its, now redacted, statement that the risk of myocarditis in young boys is 1 in 16,000, we can note that this figure is, indeed, inaccurate. The actual risk is far worse.
As reported in Science Magazine, Israeli researchers concluded that the risk of myocarditis from the Pfizer vaccine (the only vaccine currently being administered to anyone <16 years in the West) is between 1 in 3,000 and 1 in 6,000.7
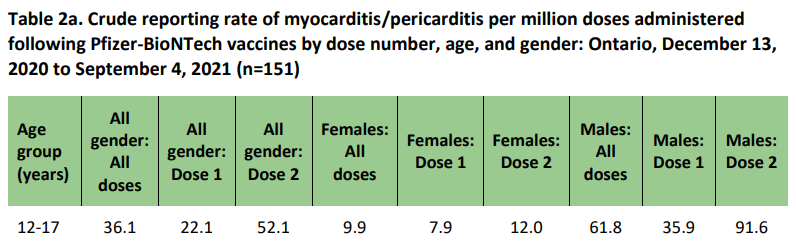
A large study from Ontario found similar findings. In 12-17 year old males, they found an incidence of 35.9 cases of myocarditis per million for Dose 1 of Pfizer and 91.6 cases per million for Dose 2. Taken together (as this is a two dose course) the risk combines to 127.5 cases per million which works out at a risk of 1 in 7,843.
As for the argument that the risk of myocarditis is greater from Covid infection than the vaccines - two points:
1. As previously shown, it is clear the vaccines do not stop people getting Covid or even getting sick. So whatever risk exists of myocarditis from Covid, taking a vaccine adds a further risk of myocarditis without necessarily eliminating the risk from Covid.
2. The risk of myocarditis from the vaccines is not less than a Covid infection. As a recent paper published in Nature Medicine Journal makes clear, the risk of myocarditis in males <40 after dose 2 of Pfizer is higher than natural infection. And it gets worse. Professor Vinay Prasad points out that while the number of people vaccinated is known, the true number of people infected with SARs-CoV-II is not. Including them all (via sero-prevalence) would significantly lower the risk profile associated with infection and the contrast with the vaccine risk would grow. Furthermore, Prasad points out that were the study authors to further refine the results to only display the risks associated with younger males (up to 24 years for instance) the greater tendency of vaccine-induced myocarditis to occur in younger people would result in an even more blunt contrast. As he succinctly concludes:
“Yes, sorry to break it to you, vaccines can have risks of myocarditis EXCEEDING risks of myocarditis from infection. Pls stop saying otherwise.”

What is perhaps most troubling about this data is that it was completely unknown before the vaccines were administered to the general public. As noted previously, the trials, which are run, administered and documented by the profit-driven vaccine companies themselves, were weak and they missed this extremely significant problem. So, what else did they miss? What else will be revealed in the coming months/years as our children fill in the blanks for these multi-billion dollar companies? Or, as one FDA voting member said during the authorisation meeting for the vaccine in the 5-11 year old cohort:
“We’re never going to learn about how safe the vaccine is unless we start giving it. That’s just the way it goes.”
Indeed. That’s just the way it goes.
7. Natural Immunity is Superior
A huge Israeli study covering 2.5 million people showed clearly that immunity acquired from infection is significantly superior to vaccine-induced immunity, offering better protection from infection and symptomatic disease. This was in relation to the Delta variant (as above, vaccine efficacy seems even less with the currently dominant Omicron). As the authors concluded:
“This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 (Pfizer-Biontech) two-dose vaccine-induced immunity.”
We are nearly two years into the Pandemic at this stage. There is a significant chance that most children have already been infected by now and acquired natural immunity. If they haven’t, they will likely catch it soon, vaccine or not, as Omicron continues to set record case numbers. As Ireland’s CMO said recently:
“It is inevitable that children will pick up this infection from household contacts in the days and weeks ahead.”8
If you vaccinated your child today, full vaccine immunity would be 5 weeks away (3 weeks between doses plus 2 further weeks before immunity is achieved as per the manufacturers). The likelihood of your child reaching that point without having already contracted Covid must be exceedingly small. So, given that they would likely have superior naturally-acquired infection, why would you pursue an inferior immunity at the cost of the risks outlined above?
8. Misplaced Trust
In 2009, following the licencing of Pandemrix by the European Medicines Agency (EMA) and its recommendation by the National Immunisation Advisory Committee (NIAC), Ireland pursued a campaign to vaccinate children against Swine Flu. Ireland’s CMO, Tony Holohan said, at the time:
“We are quite happy that this vaccine, as with all other influenza vaccines, have actually got a very good safety profile.”9
In an article headlined “Authorities insist on safety of vaccine”, Holohan stressed the importance of getting it to “young people” as quickly as possible and concluded by saying:
“We have no hesitation in recommending it.”
The HSE sounded a similar note, stating:
“As with any vaccines risks have to be balanced with the benefits and the authorities in Ireland are satisfied that the benefits from both vaccines outweigh any possible risks of side effects.”10
Pandemrix was developed quickly to address the Swine Flu epidemic but it was later withdrawn following what has been described as a “Narcolepsy Epidemic”. In Ireland alone, dozens and dozens of compensation cases went to court where children whose lives were destroyed by this vaccine were paid millions of euro by the HSE. These court cases continue right up the current day with vast sums of compensation being paid out by the Irish Government at the very time that they are in the process of rolling out another quickly produced vaccine to children.
Years after the Pandemrix scandal, the British Medical Journal conducted an investigation and clearly demonstrated that far from the claims at the time that the vaccine had been thoroughly tested, governments around the world had, in fact, made:
“various logistical and legal arrangements to shorten the time between recognition of a pandemic virus and the production of a vaccine and administration of that vaccine in the population.”
Shortcuts, I think we call them. One of which was to “provide vaccine manufacturers indemnity from liability for wrongdoing, thereby reducing the risk of a lawsuit stemming from vaccine related injury.” Indemnity from liability - sound familiar? The same thing has been used today for the Covid vaccines. Ultimately, in the case of Pandemrix, this measure did nothing to reduce the number of lawsuits, it just meant the Irish State (i.e., us) picked up the tab while the manufacturers were protected.
Perhaps the most disturbing aspect of the investigation, however, was that it showed knowledge by the manufacturers of a likely problem with Pandemrix at a time when the vaccine was still being administered and would continue to be administered for quite some time. The manufacturer, GSK, was receiving 5 times the number of reports about Pandemrix than the other vaccines - information that was not made available to the parents of children who were bringing their children forward for vaccination.
The failure of the Irish State and its Public Health Authorities was articulated most clearly by Irish TD Clare Daly, who, in addressing the Taoiseach, said:
“The Health Service Executive (HSE) decided to purchase Pandemrix and continued to distribute it even after they knew it was dangerous and untested, and before most of the public in Ireland received it.”
Or, as Tom Jefferson, epidemiologist and expert hired by one of the Pandemrix victims, said:
“The Irish government kept inviting people to get vaccinated. This was when it was quite clear that the pandemic was on the wane and it was nowhere near the catastrophe portrayed by influenza researchers, governments, industry, and the media.”
While we note the numerous parallels to the current Covid situation and the rollout of a rushed and poorly tested vaccine to children, we might consider how, in his misplaced insistence of the safety of Pandemrix, Ireland’s CMO referenced over 70 clinical studies testifying to the safety of one of its adjuvants. For the Pfizer Covid vaccine for children we have one such study - conducted by Pfizer itself. That same CMO, Tony Holohan, is still in his position today overseeing the country’s response to Covid and offering the same recommendations and assurances:
“Following advice from NIAC, which has been approved by Government, I encourage parents and guardians of those aged 12-15 years of age to register them for a vaccination as soon as the opportunity arises.”11
Ask yourself what stock you should put in the words of this man.
Conclusion
Your children are your children, nobody else’s. The decision to put them forward to receive an unapproved, rushed vaccine with zero evidence of clinical efficacy and significant evidence of risk, for a disease that bears them no realistic threat, is yours alone. It’s important to know that because considerable pressure - state, media and social pressure - will be used to point you in one direction. But there is another direction.
In America, only 15.62% of children aged 5-11 years have been fully vaccinated despite the vaccines being available there for several months.12 In Taiwan, they suspended giving 2nd doses to children aged 12-17 years because of the risk of myocarditis.13 These people aren’t wrong or inconsiderate or reckless with their children. They’re making a different decision, one which I hope I’ve demonstrated here is far from unreasonable.
The world is a complicated place. Arm yourself with information but also, if nothing else, trust your instincts - they’ve gotten you this far already.
13th Jan 2022: See here for another, very compelling, reason that recently came to light.
This is a good article detailing the bizarre situation whereby the FDA have technically fully approved a Covid vaccine but it is impossible to obtain the vaccine and the manufacturers seem to have no intent to produce it. https://theohiostar.com/2021/12/15/exclusive-ohios-largest-hospital-system-still-distributing-pfizer-covid-19-vaccine-not-fully-approved-by-fda/
https://www.statnews.com/2021/09/20/pfizer-covid-19-vaccine-children/?utm_content=buffer45f59&utm_medium=social&utm_source=twitter&utm_campaign=twitter_organic
https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-by-Sex-and-Age/9bhg-hcku/data
https://www.nejm.org/doi/full/10.1056/NEJMsr1804754
https://metro.co.uk/2021/09/17/more-than-half-of-people-suffering-from-long-covid-might-not-have-it-15272884/
https://www.dailymail.co.uk/health/article-9839697/Fauci-says-CDC-changed-mask-guidance-vaccinated-people-spread-Indian-Delta-variant.html
https://www.science.org/content/article/israel-reports-link-between-rare-cases-heart-inflammation-and-covid-19-vaccination
https://www.irishtimes.com/news/health/inevitable-children-will-get-covid-19-in-households-in-weeks-ahead-says-holohan-1.4768436
https://www.irishtimes.com/news/authorities-insist-on-safety-of-vaccine-1.847977
ibid.
https://www.breakingnews.ie/ireland/chief-medical-officer-urges-parents-to-register-children-for-covid-19-vaccine-1163921.html
https://usafacts.org/visualizations/covid-vaccine-tracker-states/
https://www.taiwannews.com.tw/en/news/4340862
I only need one reason not to vaccinate my children. Because I’m their mother and it’s my job to keep them safe. These are not vaccines. They’re injections. And they are not safe. So I say no.
I wish that the government and the health system would respect our wishes. Even if they were not harming people it is still our right to say no without being punished for it. And this latest stack from Steve Kirsh… well I have no words.
https://stevekirsch.substack.com/p/welcome-to-the-new-normal-13-year
Excellent piece, Damian.